Forget about twitches, it is all about CMAP
Oct 5, 2023
By Linnea Troeng, Global Product Manager at Senzime

When it comes to measuring muscle activity and neuromuscular blockade during anesthesia, forget about twitches. The real focus should be on Compound Muscle Action Potential (CMAP).
In this post, I will tell you why.
A neuromuscular assessment can be subjective or objective. Visual or tactile assessment of the twitch responses is considered qualitative (subjective) neuromuscular assessment because the clinician guesses the degree of fade or recovery, instead of measuring the strength of responses. The result is therefore subjective and unreliable, regardless of the clinician’s level of experience or training. Clinically meaningful degrees of neuromuscular blockade can only be measured using a quantitative, objective, monitoring device. A residual neuromuscular block of TOFR > 0.4 cannot be reliably detected by tactile or visual means even by an experienced clinician.
Clinical tests, such as 5-s head-lift, tidal volume or grip strength do not guarantee complete resolution of neuromuscular block and should not be used to make clinical decisions about the adequacy of neuromuscular function. This is where quantitative neuromuscular monitors enter the game, for improved patient safety.
Quantitative monitors measure and quantify the degree of neuromuscular blockade and display the results numerically. Quantitative assessment of the train-of-four fade by neuromuscular transmission monitors is the only suitable method to identify low but clinically meaningful levels of residual neuromuscular block. To determine whether full recovery of neuromuscular function has occurred at the time of tracheal extubation, quantitative monitors are required.
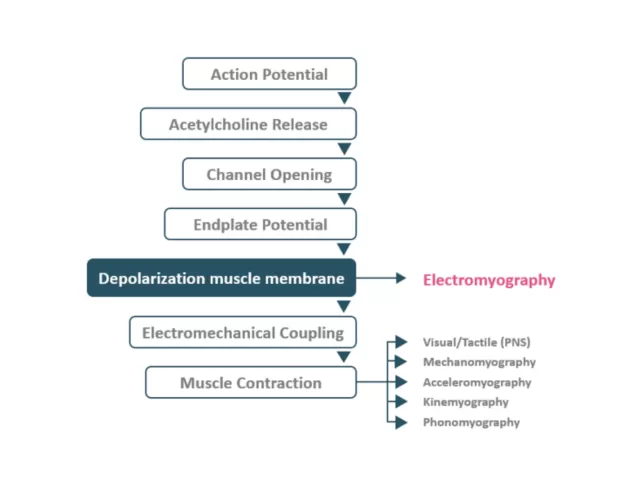
Electromyography (EMG) measures the electrical signal during depolarization at the neuromuscular junction. The compound muscle action potential (CMAP) is the first electrical signal that can be measured after neuromuscular transmission.
Other methods, such as subjective monitoring (e.g. PNS) and Acceleromyography (AMG), measure the contractile response through movement of the muscle itself. Those methods are prone to errors since the register of movement of the thumb requires free movement of the hand. In many surgeries, the arm is tucked under drapes, and free thumb movement is prohibited.
Unlike other technologies, EMG does not rely on physical movement to measure function. This makes it a superior indicator of pure neuromuscular function.
So, if you want to accurately measure muscle blockade and recovery during surgery, forget about twitches and focus on CMAP and EMG.
This method provides a more precise and reliable way to assess muscle function during surgery.

TetraGraph is the quantitative TOF monitor of choice by many clinicians worldwide, powered by the 7th generation EMG algorithm.
With Prof. Lars I. Eriksson, Professor and Academic Chair of Anesthesiology and Intensive Care, at Karolinska institute in Stockholm.