New guidelines pave the way for safer neuromuscular block management in pediatric anesthesia
April 22, 2026 (first published June 12, 2025)
By AnnaMaria Tahlén, Global Digital & Brand Marketing Manager

In this blog, we will discuss the need for monitoring in pediatric anesthesia and how the new European guidelines could help drive safer anesthesia practice worldwide.
Pediatric-specific guidelines have been released, recommending the use of quantitative neuromuscular monitoring during anesthesia in children (1). The original presentation, made at the Euroanaesthesia 2025 congress, marked a significant step toward improving perioperative safety in pediatric patients.
It is encouraging to see that the final guidelines are now published and are the first to specifically advocate for this practice in pediatrics. The new guidelines also explicitly prefer electromyography (EMG) over acceleromyography (AMG).
The need for neuromuscular monitoring in pediatric anesthesia
Each year, approximately 10-12 million major pediatric surgeries worldwide involve the use of neuromuscular blocking agents (NMBAs). For the United States alone, it’s close to 3 million cases per year. NMBAs are commonly used to facilitate endotracheal intubation and optimize surgical conditions.
However, without objective quantitative monitoring, up to 40% of pediatric patients may experience residual neuromuscular block (rNMB) during the postoperative period. Residual paralysis remains one of the most common and preventable causes of postoperative respiratory complications in anesthesia practice. (2,3).
Despite the well-known risks of residual paralysis, pediatric anesthesia has historically relied on qualitative monitoring and often no monitoring at all, due to the lack of pediatric-specific sensors.
The good news is that electromyography (EMG)-based quantitative train-of-four (TOF) monitoring is now available and offers an accurate and reliable option for monitoring in pediatrics.
In the new guidelines, EMG is explicitly identified as the preferred technology for quantitative neuromuscular monitoring, reflecting its ability to measure the electrical activity of the muscle directly rather than relying on movement, which can be influenced by positioning or surgical conditions.
Key points of the new pediatric guidelines
The guidelines were first presented as part of the session Hot topics in ESAIC Guidelines (part II) at Euroanaesthesia 2025, where Dr. Francis Veyckemans highlighted a clear need for pediatric-specific guidance.
Dr. Francis Veyckemans pointed out that current practices lag behind adult standards—especially concerning the use of NMB monitoring. (4)
Now with the published guidelines (1), here are the key points when it comes to monitoring:
- We recommend the use of a neuromuscular blocking agent (NMBA) to facilitate tracheal intubation in children under general anaesthesia in the operating room when maintaining spontaneous breathing is not required.
- We recommend, whenever an NMBA is used, quantitative neuromuscular monitoring be applied to modulate the level of neuromuscular block and to rule out a residual neuromuscular block before extubation.
- We suggest electromyography-based rather than acceleromyography-based quantitative neuromuscular monitoring and calibrating the device before administering a NMBA.
One of the most concerning practices in pediatric anesthesia today is the administration of sugammadex without a quantitative TOF monitor. Sugammadex is a selective relaxant-binding agent that encapsulates NMBA molecules, allowing rapid reversal of neuromuscular block.
However, without quantitative neuromuscular monitoring, studies have shown that 87% of patients may receive an excessive dose and 13% an insufficient dose, increasing the risk of recurarization or prolonged paralysis.(5)
Encouragingly, advancements in monitoring technology, especially EMG-based systems, are now making it more feasible to apply quantitative monitoring in infants and children. These innovations have the potential to improve perioperative care and patient safety.
When it comes to NMBAs and reversal agents, the new pediatric guidelines (1) state:
- We recommend sugammadex over neostigmine for the reversal of aminosteroid NMBA in children due to its faster recovery time, shorter time to extubation, and more effective reversal of moderate and deep block.
- For rapid sequence induction and intubation, we recommend using rocuronium rather than succinylcholine.
- To prevent residual neuromuscular block or recurarisation, we suggest avoiding excessive doses of rocuronium and using systematic quantitative neuromuscular monitoring to ensure adequate recovery before extubation.
- If an NMBA is necessary, rocuronium or vecuronium is preferred, as they can be reversed with sugammadex.
- Regardless of the NMBA used, its dose should be titrated according to the child's level of NMB, as evaluated with quantitative neuromuscular monitoring.
Guidelines to drive the change for patient safety
The adult neuromuscular monitoring guidelines were published in late 2022, nearly simultaneously by both the American Society of Anesthesiologists (ASA) and the European Society of Anesthesia and Intensive Care (ESAIC).
Since then, these guidelines have significantly raised awareness about the importance of neuromuscular monitoring and contributed to a broader adoption of quantitative techniques in clinical practice.
Can we expect a similar shift in pediatric anesthesia with the new pediatric guidelines? The hope—and expectation—is yes.
The pediatric guidelines from ESPA and ESAIC have the potential to drive change in clinical practice, moving toward safer, evidence-based anesthesia care.
Now it’s time for hospitals, clinicians, and equipment providers to start exploring EMG-based monitoring technology, to make sure every pediatric patient can benefit from the same standards increasingly seen in adult care.
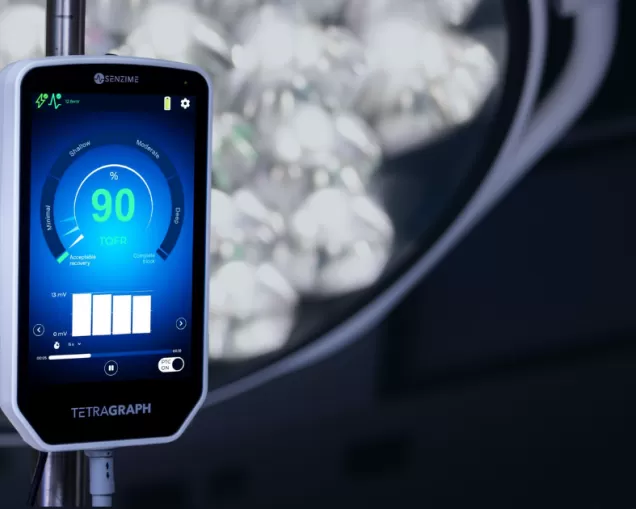
How TetraGraph can help advance pediatric anesthesia
The next-generation TetraGraph system, equipped with the TetraSens Pediatric sensor, delivers real-time, precise EMG-based assessment of neuromuscular function.
Unlike traditional acceleromyography (AMG) monitors, TetraGraph eliminates the need for free-moving muscles, making it ideal for pediatric patients, especially during tucked-arm laparoscopic and robotic surgical cases.
TetraSens Pediatric is made from soft, flexible materials and is an FDA-cleared EMG sensor with a separate and specific pediatric indication from one month old (defined as 28 days).
Contact our team to explore this solution or explore it at our pediatric page.
Key insights from this blog
- New European guidelines for pediatric anesthesia recommend quantitative neuromuscular monitoring to improve safety in children receiving neuromuscular blocking agents.
- New guidelines recommend electromyography (EMG) over acceleromyography (AMG) for monitoring pediatric patients.
- Up to 40% of pediatric patients experience residual neuromuscular block (rNMB) postoperatively posing serious risks when monitoring is absent or qualitative.
- TetraGraph, with its TetraSens Pediatric sensor, delivers an advanced EMG-based monitoring solution that positions clinicians to meet the new pediatric guidelines with confidence.
AnnaMaria Tahlén, Global Digital & Brand Marketing Manager at Senzime
If you have any further questions or require additional information, feel free to contact me and my colleagues.
References
- Veyckemans, Francis; Debouche, Sophie; Kaufmann, Jost; Disma, Nicola; Amigoni, Angela; Bonatti, Giulia; Christensen, Michelle Icka; Engelhardt, Thomas; Fuchs, Alexander; Fuchs-Buder, Thomas; Hansen, Tom G.; Karlsson, Jacob; Kleine-Brueggeney, Maren; Lusardi, Andrea Clarissa; Riva, Thomas; Salaün, Jean-Philippe; Saldien, Vera; Saynhalath, Rita; Scavenius, Mikkel; Schmartz, Denis; Vanlinthout, Luc E.; Vieira, Ricardo Carlos; von Ungern-Sternberg, Britta S.; Romero, Carolina S.; Afshari, Arash. 2025 ESAIC and ESPA Guidelines on neuromuscular block in anaesthetised children: Indications, monitoring and reversal. European Journal of Anaesthesiology 43(4):p 295-323, April 2026. | DOI: 10.1097/EJA.0000000000002357
- Faulk DJ, Karlik JB, Strupp KM, Tran SM, Twite M, Brull SJ, Yaster M, Austin TM. The Incidence of Residual Neuromuscular Block in Pediatrics: A Prospective, Pragmatic, Multi-institutional Cohort Study. Cureus. 2024 Mar 18;16(3):e56408. doi: 10.7759/cureus.56408. PMID: 38638790; PMCID: PMC11024486.
- Engelhardt T, Virag K, Veyckemans F, Habre W.Airway Management in Paediatric Anaesthesia in Europe – Insights from APRICOT (Anaesthesia Practice in Children Observational Trial): A prospective multicentre observational study in 261 hospitals in Europe. Br J Anaesth 2018, 121; 66-75.
- Dr. Francis Veyckemans (Brussels, Belgium), May 26, ESAIC Guidelines (C) on muscle relaxation in anaesthetised children: indications, monitoring, and reversal, Hot topics in ESAIC Guidelines (part II), Euroanaesthesia 2025, Lisbon, Portugal.
- Bowdle TA, Haththotuwegama KJ, Jelacic S, Nguyen ST, Togashi K, Michaelsen KE. A Dose-finding Study of Sugammadex for Reversal of Rocuronium in Cardiac Surgery Patients and Postoperative Monitoring for Recurrent Paralysis. Anesthesiology. 2023 Jul 1;139(1):6-15. doi: 10.1097/ALN.0000000000004578. PMID: 37027807.